60 yr old female with fever, SOB and cough from 2 weeks.
Supriya
Sanjay
Amrutha
Mohitha
Sowmya
Dr Durga Krishna pgy1
Dr Ajith Kumar pgy2
Dr Laxma Reddy pgy3
Dr Manasa pgy3
Dr Vijayalakshmi Ast.prof.
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box is welcome.
A 60yr old female presented with c/o
Fever 15 days back
cough from 15 days
Shortness of breath from 10 days.
Patient was apparently asymptomatic 15 days back, then she developed fever with chills and rigors, continuous and cough which was non productive.
She went to a private hospital and was diagnosed with typhoid and used medication for 4 days. Her fever subsided in 4 days.
She developed shortness of breath 10 days back.
She got a chest XRay done and was found to have pneumonia. They were referred to a government hospital.
Patient went to the government hospital and got admitted in the government hospital for 7 days and was treated but her symptoms were not relieved. She was referred to our hospital for further evaluation.
PAST HISTORY:
No h/o HTN,DM,TB,ASTHMA,CVA,CAD.
No past surgeries
PERSONAL HISTORY:
Good appetite
Mixed diet
Sleep adequate
Regular bowel and bladder movements.
No addictions
No know allergies.
GENERAL EXAMINATION:
Patient is conscious, coherent, cooperative.
No pallor, icterus, cyanosis, clubbing, pedal edema, generalised lymphadenopathy.




Vitals
Afebrile.
Bp-120/80 mmhg
PR-84 bpm
RR- 35cpm
spo2-99%
CVS-
Apical impulse in the 5th ICS medial to MCL.
S1 S2 heard.
No murmurs.
RS-
Inspection:
Resp rate- 35/min
Shape of chest: elliptical.
AP- 17cm
Transverse- 25cm
Breathing pattern: thoraco-abdominal
Equal B/l chest movements.
No scars, sinus, engorged veins.
Palpation:
Trachea central.
Chest expansion - equal on both sides.
TVF decreased in infra scapular and infra axillary areas.
Auscultation:
BAE+
Tubular breath sounds in b/l lower lobes.
Crepts heard in B/L lower lobes along with ronchi.
Fine crepts in b/l infra axillary area and infra scapular areas.
P/A-
Soft.
Non tender.
No organomegaly.
Bowel sounds +
CNS- NAD.
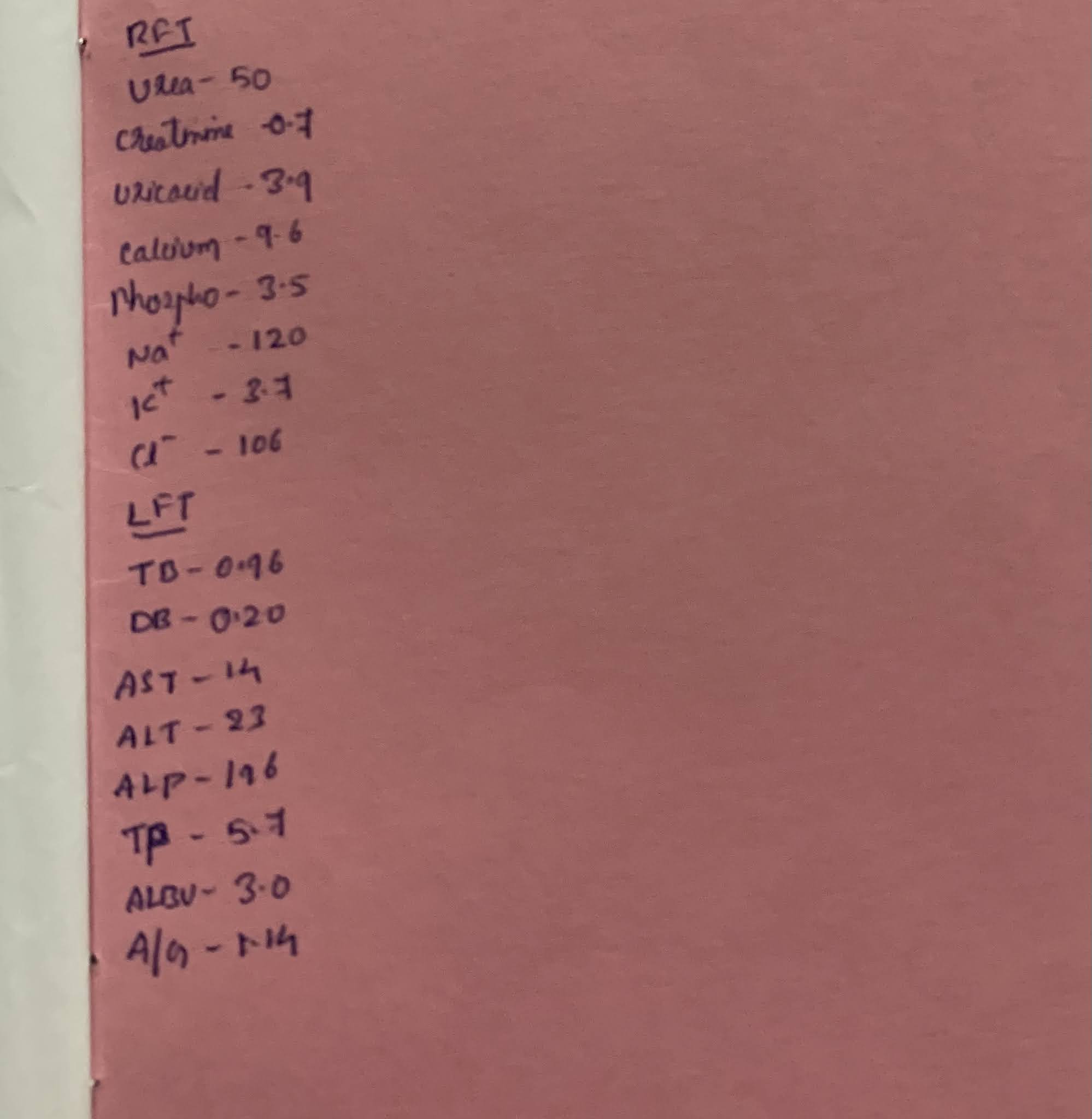
INVESTIGATIONS:




DIAGNOSIS:
PNEUMONIA (?COMMUNITY ACQUIRED)
RIGHT LOWER LOBE CONSOLIDATION.
TREATMENT:
1. Inj. AUGMENTIN 1.2g/IV/TID
2. Tab. AZITHROMYCIN 500mg/ PO/OD
3. Inj. PAN 40mg IV/OD
4. Inj. ZOFER 4mg/IV/SOS.
5. Inj. HYDROCORT 100mg IV/BD.
6. NEBULISATION WITH BUDECORT AND DUOLIN 4th hrly.


Really I feel happy to see this useful blog, Thanks for sharing such a nice blog.
ReplyDeleteGeneral Medicine in Greater Noida
Thank you for sharing this blog. Necessary first aid should be given as soon as the injury occurs. The first aid that can do so is to use it greatly to heal our wound quickly. Use seeskin plus collagen sponge dressing to cure your wounds fast and safe.
ReplyDeleteThank you for giving this article. Injury and ulcers in the body can have very bad effects on our body if not properly maintained. I'm sure kci vac consister 300ml/500ml with gel a pioneer in wound healing.
ReplyDeleteThank you for the article. We are primarily involved in providing the medicines you need to heal your wounds.
ReplyDeleteseeskin ultrathin collagen sheet