55 yr old with weakness of left upper and lower limb.
Interns
M Supriya
Sowmya Kota
Mohitha
Amrutha
Sanjay
Dr Durga Krishna PGY1
Dr Ajith Kumar PGY2
Dr Laxma Reddy PGY3
Dr Manasa PGY3
Dr Vijayalaxmi (Ast prof.)
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box is welcome.
A 55 yr old female presented with weakness of the left upper limb and left lower limb from 1 week.
C/o slurring of speech from 1 week
Deviation of mouth to the right side from 1 week
C/o reduced sleep, reduced appetite, self talking from 2 months
H/o wandering episodes from 1 and half month.
Patient was apparently asymptomatic 22 yr back then she started going out and sitting alone and had wandering episodes. She was taken to a psychiatrist where she was diagnosed with psychosis(NOS) and she was on medication from then and was visiting the psychiatrist and was normal for about 20 yrs and since lockdown she was not using any medication.
Patient has reduced sleep, reduced appetite, self talking from 2 months.
She had 2 wandering episodes 1 and half month back.Patient used to come back home on her own sometimes and sometimes her relatives had to look for her and bring her back.
Patient has only liquid diet from 15 days.
She is unable to hold water in her mouth and it drips from her mouth when she tries to drink.
She has weakness of left upper limb and lower limb from 1 week, slurring of speech from 1 week and deviation of mouth to right side and patient was referred to kims for further evaluation.
PAST HISTORY:
No h/o HTN, DM, TB, Asthma,Epilepsy.
K/c/o psychosis NOS from 22 yrs and on regular medication except for the last 2 months
PERSONAL HISTORY:
Patient has a reduced appetite, vegetarian diet, reduced sleep, regular bowel and bladder movements, no addictions
No known allergies.
O/E-
Patient is in altered sensorium at admission.
No pallor, icterus, cyanosis, clubbing, generalised lymphadenopathy.
Edema present in the left upper and lower limbs.



VITALS
Bp-120/80mmhg
Pr-90bpm
Rr-20cpm
Spo2-98%
Grbs-141
SYSTEMIC EXAMINATION:
CVS- S1S2 +
No murmurs
RS-BAE+
NVBS+
P/A- soft,non tender,
no organomegaly.
CNS-
Conscious
Slurred speech
Pupils bilateral NSRL
No meningeal signs
Cranial nerves:
Facial nerve-
Forehead wrinkles present.

Loss of nasolabial fold on left side.

Motor system-
Right. Left
Tone - UL Hypertonic Hypotonic
LL Hypertonic Hypotonic
Power- U/L- 3/5. 0/5
L/L- 3/5. 0/5
DTR- Biceps. ++ +++
Triceps. ++ +++
Supinator + ++
Knee. ++ +++
Ankle. + ++
Plantar- Flexion Flexion
Sensory system- intact in both sides.
Cerebellar system- unable to examine.
INVESTIGATIONS:










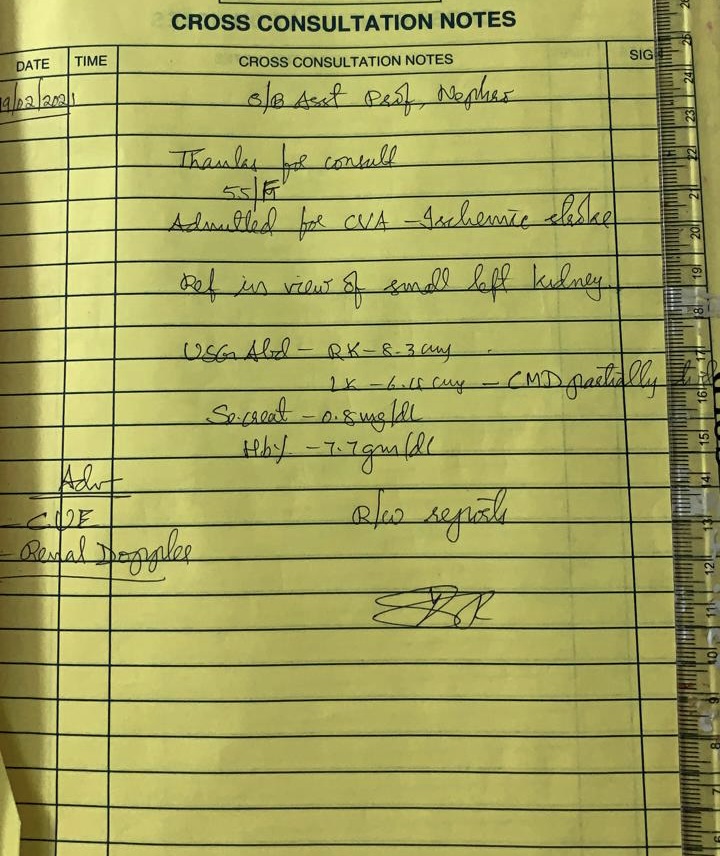
DIAGNOSIS:
CVA with left sided hemiplegia with left LMN type facial palsy with psychosis Nos.
Acute infarct in the left temporal, frontal, right centrum semiovale.
TREATMENT:
1. Ryle’s tube feeding with 100ml milk and 100 ml water 2nd hrly.
2. Tab Aspirin 75mgRT/OD.
3.Tab Atorvas 40mg RT/OD/HS.
4. Inj Pan 40mg IV OD
5.Tab Olanzapine 5mg RT/OD
6. Physiotherapy of left upper and lower limb.



Comments
Post a Comment