38 years male with acute on chronic pancreatitis.
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box is welcome.
Here is a case i have seen:
A 38 year old male who is cab and lorry driver by occupation, resident of Anumula came to general medicine OPD with complaint of pain abdomen from 20 days.
HOPI-
Patient was apparently asymptomatic 9 years ago then he developed pain in the epigastrium which was sudden in onset and progressive, nonradiating, no aggravating and relieving factors. H/O alcohol intake prior to the episode for 2 months regularly(360 ml). No H/O vomitings.
Patient was diagnosed with Hypertension and Diabetes Mellitus at the same time. Stopped alcohol intake for 4 years after this episode. Started consuming alcohol again after 4 yrs.
Now similar complaint of pain in the epigastrium and left hypochondrium from 20 days. Gradual in onset, progressive, nonradiating, no aggravating and relieving factors. For the pain he initially took medication from a local pharmacy for 15 days but the pain did not subside.
Patient went to a government hospital where he was referred to kims for further evaluation.
H/O reduced intake of food due to pain abdomen.
H/O binge alcohol intake 2 months ago for 40 days regularly(360ml/day).
He did not consume alcohol in the last 2 months.
No H/O fever,vomitings,loose stools.
PAST HISTORY-
K/C/O Hypertension from 9 yrs and is on Tab.Telma 40 and Tab.Hydrochlorothiazide 12.5mg.
K/C/O DM from 9 yrs and is on TAB. Glimiperide and Tab.Metformin.
PERSONAL HISTORY-
Normal appetite.
Mixed diet.
Alcoholic intake from 15yrs, about 360ml per day.
Smoker from 15 years, 1 pack per day.
Stopped consuming alcohol and smoking 2 months ago.
GENERAL EXAMINATION:
Patient was consious, coherent, cooperative; oriented to time,place,person.
No pallor, icterus, clubbing, cynosis, lypmhadenopathy, pedal edema.
VITALS:
BP- 130/90 mmhg sitting position right arm
PR-95bpm, regular rhythm
RR- 17cpm
SpO2- 97%
SYSTEMIC EXAMINATION-
CVS- S1S2 heard, no murmurs.
RS- BLAE + NVBS+
CNS- No FND.
P/A-
Inspection:
Shape of abdomen-normal
Umbilicus central,inverted
No engorged veins, scars, sinuses.
No visible pulsations.
Palpation:
No local rise of temperature.
Tenderness seen in the epigastrium and left hypochondrium.
No guarding.
No rigidity.
No organomegaly.
Auscultation:
Bowel sounds heard.
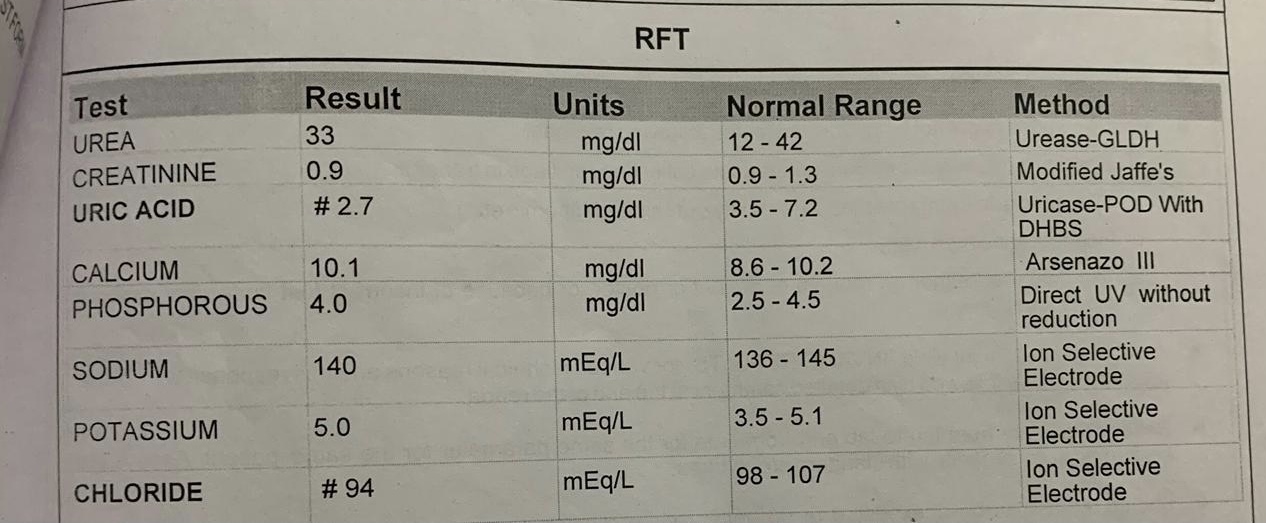
INVESTIGATIONS:
21/1/2021
Hemogram

LFT


ABG

Serum amylase




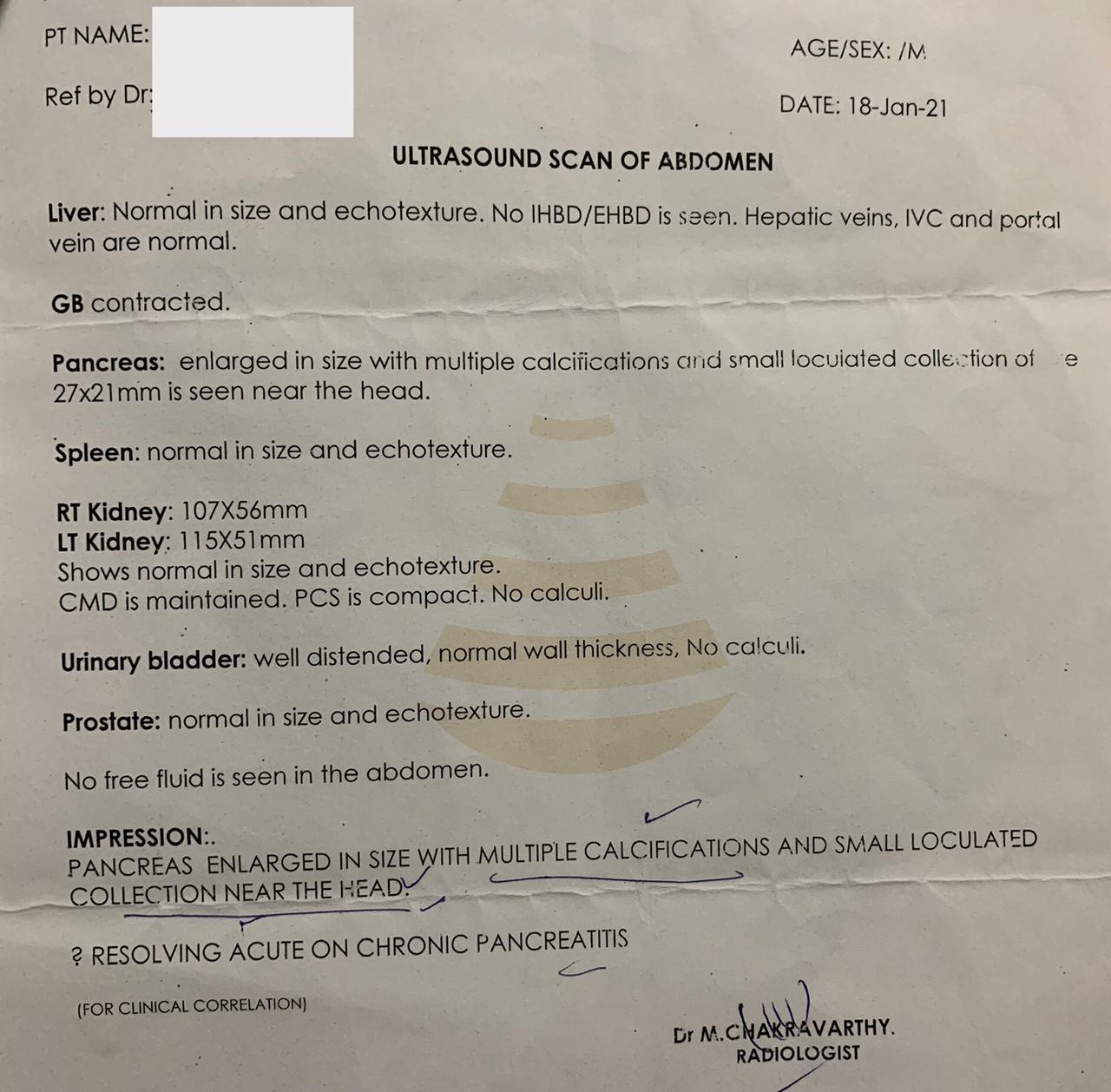

CECT Abdomen


DIAGNOSIS:
ACUTE ON CHRONIC PANCREATITIS WITH HYPERTENSION WITH DIABETES MELLITUS
TREATMENT:
1.NBM till further orders.
2.IVF- 1 NS and RL at 100ml/hr
3.Inj.Pan 40mg IV/OD
4.Inj. Ceftriaxone 1GM IV/BD
5.Inj. Tramadol 1 ampule in 100 ml NS IV/OD
6.Inj.Optineura 1 ampule in 100ml NS IV/OD
7.Strict I/O monitoring
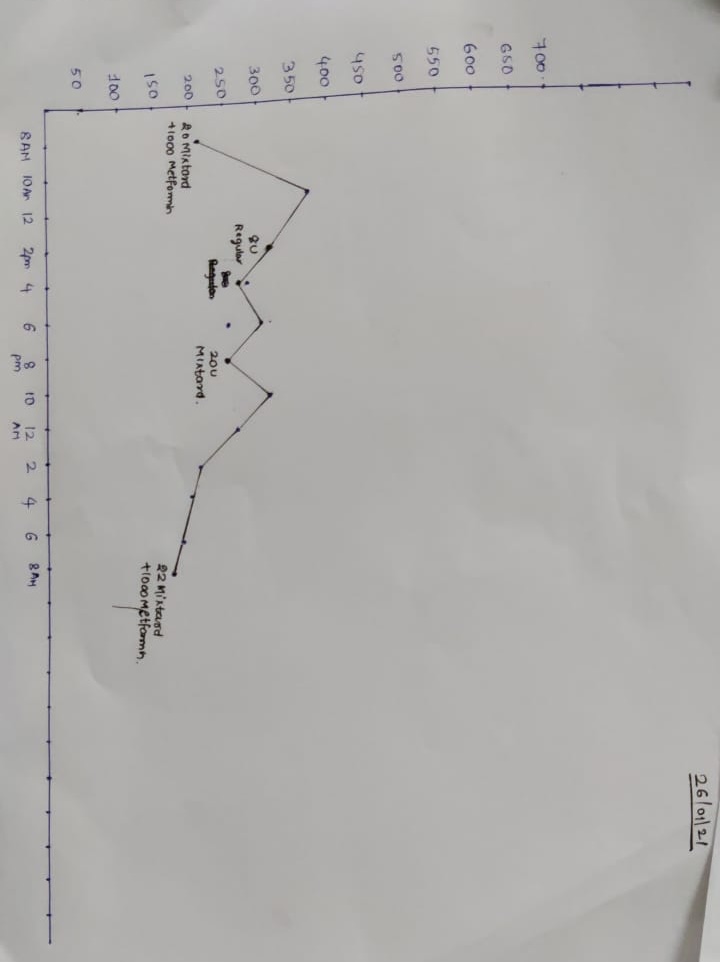
8.GRBS monitoring 4th hrly.
9.Inj.HAI SC according to sliding scale.


Comments
Post a Comment